Mada za sehemu hiiGaseous Exchange And RespirationMada 4
- Gaseous Exchange in Mammals.
- Respiration
- Glycolysis
- Kreb’s Cycle
Gaseous exchange is the movement of oxygen and carbon dioxide between the organism and its environment at the respiratory surfaces.
Oxygen goes in and carbon dioxide goes out – these gases move in and out through diffusion.
Respiratory surfaces are surfaces on which gaseous exchange takes place.
In case of unicellular organisms, gaseous exchange usually takes place throughout the whole body, i.e., the cell and the distance through which gases have to travel is small. In large multicellular organisms there are well developed respiratory systems through which gases move in and out of the organism from and to the external environment.
- Skin – amphibians, e.g., toads/frogs.
- Lungs – chordata and aves.
- Lung books – arachnida, e.g., scorpion.
- Gills – external gills, e.g., larval amphibians and crustaceans. Internal gills, e.g., fishes.
- Tracheal in insects – tracheae receive and give out gases directly.
- Buccal cavity – amphibians.
- They should be moist in order to dissolve the gases (gases diffuse better when they are in solution). They must also be permeable.
- They must have large surface area to volume ratio to take in or take out gases.
- They must be thin to minimize the distance through which the gases have to travel.
- They must have a respiratory pigment, e.g., haemoglobin – iron-containing pigment; haemocyanin – copper-containing pigment.
- Ventilation – there must be a constant supply of air or water to the respiratory surface because as oxygen diffuses inwards it tends to be depleted immediately next to the gaseous exchange surface. Therefore, the supply of oxygen from the external environment can be much more efficiently replaced. A flow of this kind is called ventilation.
- They must be highly vascularised, i.e., supplied with blood capillaries (vessels) to transport the gases.
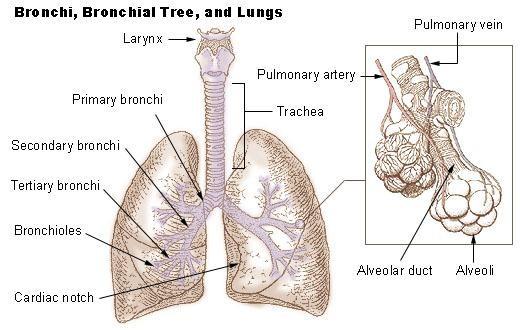
The organ of gaseous exchange is the lung and the respiratory surfaces are the alveoli. The gaseous exchange takes place along the respiratory tract.
- Air enters the body through the nose.
- It then moves to the trachea.
- The trachea branches into 2 bronchi (bronchus).
- The bronchi further branch into several bronchioles. (The bronchioles contain less cartilage than the bronchi).
- The respiratory surfaces are the alveoli where gaseous exchange takes place.
- The walls of the passage/tract are lined with ciliated epithelial cells (have hair-like structure) and goblet cells which produce mucus. The mucus traps foreign particles like dust, bacteria which enter the respiratory tract with air. The vibration of the cilia sweeps the trapped particles backwards into the pharynx and then they are swallowed.
- Presence of hair in the nasal cavity. This traps the particles coming in along with air. They act as filters of dust and foreign particles.
- The mucus produced not only traps the foreign particles but also moistens the respiratory tract.
- Presence of numerous blood capillaries whose blood provides a continuous supply of moisture to air to keep it moist before it reaches the alveoli and also supplies heat to warm the incoming air so that the air is warmed up to body temperature so that the alveoli are not damaged.
- The trachea remains open for continuous inhalation and exhalation. This is made possible by the cartilage which also gives strength to the passage. Presence of collagen and elastic fibres in the alveoli which allow the alveoli to expand and recoil easily.
- Special cells in the walls of the alveoli produce a chemical called surfactant. Its roles are:
- It prevents alveoli walls from sticking together.
- It kills any bacteria that make it to the alveoli.
- It speeds up the transportation of carbon dioxide and oxygen between the air and the liquid lining of alveoli.
- It lowers the surface tension of the liquid layer lining the alveoli.
- Presence of macrophages on the surface of the alveoli which keep them clean by scavenging the bacteria that reaches the alveoli. Macrophages are actually white blood cells.
The nasal cavity
The nasal passages have a relatively large surface area but no gaseous exchange takes place here. The passages have a good blood supply and the lining secretes mucus and it is covered by hair. The air is cleaned, moistened and warmed as it passes through the nasal cavity.
The trachea
The trachea is a major airway, heading down to the chest cavity. It is lined with columnar epithelial cells. In the layers below the epithelium are mucus-secreting cells (goblet cells). The inner side of the columnar cells is lined with air.
- The trachea is made up of cartilage rings which prevent them from collapsing. The cartilage rings are incomplete to allow the easy passage of food down the oesophagus that runs below the trachea.
- The cartilage rings are C-shaped.
The bronchus
- The trachea divides into two bronchi within the chest cavity, one leading to the left lung and the other leading to the right.
- The bronchi are very similar to the trachea in structure, only that they are narrower.
- The left bronchus divides into two while the right bronchus divides into three.
The bronchioles
The bronchioles are much smaller than the bronchi and there are many of them, decreasing in size as they go down to the alveoli. Larger bronchioles have cartilage rings unlike those which are smaller. These small bronchioles collapse quite easily as the bronchioles get smaller. The lining epithelium changes from columnar to flattened cuboidal cells making diffusion more likely.
The alveoli
The tiny bronchioles terminate into millions of microscopic air sacs or alveoli in grape-like clusters.
- The alveoli are 0.1 mm in diameter and they are 0.5 mm in thickness.
- They have elastic walls lined (supplied) with blood capillaries from the pulmonary artery.
- The alveoli are made up of squamous epithelial cells which facilitate diffusion because they have a large surface area and are thin, reducing the distance through which gases travel.
- The capillaries which run close to the alveoli also have walls which are only one cell thick, creating the best possible conditions for gaseous exchange. Between the capillaries and the alveolus is a layer of elastic connective tissues which holds them together.
- The elastic elements in the tissue help to force air out of the stretched lungs; this is known as elastic recoil of the lungs.

- External intercostal muscles contract and internal intercostal muscles relax.
- The ribs move upwards and outwards (anteriorly and ventrally).
- The diaphragm muscle contracts and flattens.
- These two movements of the ribs and diaphragm cause the volume of the thoracic cavity to increase and therefore the pressure inside it falls.
- The pressure inside the lungs is lower than that of the atmosphere.
- This causes air to rush into the lungs from the exterior.
- Breathing in is an active process but breathing out is largely passive.
- Internal intercostal muscles contract and external intercostal muscles relax.
- The ribs move downwards (posteriorly) and inwards (dorsally).
- The diaphragm muscle relaxes and resumes its dome shape.
- These movements cause the volume of the thoracic cavity to decrease and therefore pressure inside increases.
- This causes air to be forced out of the lungs as their elastic walls recoil.

There are two ways in which oxygen is transported to the respiring cells. It is carried in the blood in two forms:
- Dissolved oxygen Oxygen is dissolved in the plasma then transported to the respiring cells. It is a simple physical solution. About 2% of the oxygen in the body is transported in this way.
- Chemical form It is transported in combination with haemoglobin. About 98% of the O₂ in the body is transported in this way.
The chemical form
Oxygen is transported in combination with haemoglobin.
Haemoglobin is a protein that consists of four subunits: 2 α chains and 2 β chains. Each of these four subunits contains a special pigment or haem group.
The haem group has an iron atom located at its centre. A single Fe atom binds one molecule of oxygen (O₂). One molecule of haemoglobin therefore combines reversibly with up to 4 molecules of oxygen.
Haemoglobin is found in the red blood cells. It has high affinity for oxygen. It combines readily with oxygen. Different kinds of oxyhaemoglobin can be formed as follows:

The four oxyhaemoglobin types differ according to the degree of dissociation. Hb₄O₈ dissociates to release O₂ more readily than Hb₄O₆, and Hb₄O₆ dissociates more readily than Hb₄O₄, and so on.
The degree of dissociation is represented by a character sigmoid (S-shaped) curve called the oxygen dissociation curve.
An oxygen dissociation curve is a curve in which the percentage saturation of haemoglobin is plotted against the oxygen concentration (partial pressure).


- Myoglobin is another respiratory pigment in vertebrates.
- It consists of a single polypeptide chain and a single haem group.
- It has an oxygen dissociation curve displaced to the left of haemoglobin.
- This means it has higher (greater) affinity for oxygen.
Diving vertebrates
E.g., seals, whales, dolphins.
The duration of a single dive in seals rarely exceeds 20 minutes, whereas that of sperm whale may extend to 75 minutes. Bottlenose dolphins have been known to dive for up to two hours.
- The remarkable ability of these mammals to endure such long periods without replenishing the air supplies is a result of:
- A large total volume of blood.
- An increased concentration of RBC.
- Greater haemoglobin concentration.
- Reduced sensitivity to blood pH.
- Muscles rich in myoglobin.
- Reduction in cardiac output.
- Restriction of blood supply to vital organs.
- Tolerance to high lactate levels (muscles respire anaerobically, thus accumulation of lactic acid, but they can tolerate lactic acid which would cause fatigue and cramps in other mammals).
- Reduction of metabolic rate during diving.
- Larger tidal volume.
- Lungs may be entirely collapsed to allow exchange of air (they have few ribs attached to the sternum, making the ribcage more flexible, permitting it to collapse partially when under pressures experienced during a deep dive).
High altitude dwellers
The amount of oxygen at high altitude levels is the same as that at sea level. The respiratory problems associated with living at high altitude levels are a result of reduced pressure; it means it is more difficult to load the haemoglobin with O₂ effectively. Some human settlements exist at high altitudes and the inhabitants have become acclimatised/adapted to living in conditions of low atmospheric pressure. The acclimatisation involves:
- Adjustment of blood pH.
- Increased oxygen uptake – more O₂ is absorbed by the lungs as a result of an improved capillary network in the lungs and deeper breathing.
- Improved transport of O₂ to the tissues – this results from:
- Increased RBC concentration (45% – 60% of total blood volume).
- Changes in haemoglobin affinity for oxygen – the oxygen dissociation curve is shifted to the right to facilitate release of O₂ to the tissues.
- Increased myoglobin level in muscles – with its higher affinity for O₂, this facilitates the exchange of O₂ from blood to the tissues.
The transport of CO₂ is closely linked with the transport of O₂. CO₂ is more soluble in H₂O than O₂, but its transport in solution is inadequate to meet the needs of most organisms (vertebrates).
CO₂ is transported in three ways from the tissues (respiring cells) to the gaseous exchange surfaces:
- Aqueous solution – about 5% of the CO₂ is transported in solution in the blood plasma. CO₂ is directly dissolved in blood; it occurs in the blood plasma.
- In combination with haemoglobin – around 10% of CO₂ combines with the amine group in the four polypeptide chains which make up each haemoglobin molecule. It occurs in the RBC. CO₂ is transported in the form of carbamino haemoglobin (HbCO₂).
- In form of hydrogen carbonate (HCO₃⁻) – 85% of the CO₂ produced by tissues combines with water to form carbonic acid.

This reaction is catalysed by a zinc-containing enzyme called carbonic anhydrase.
The carbonic acid dissociates to form hydrogen carbonate ions.
The fate of hydrogen ions (H⁺)
The H⁺ combines with haemoglobin which loses its O₂. The O₂ so released from the Hb diffuses out of the RBC, through the capillary wall and tissue fluid, into the respiring tissues. Thus, the more CO₂, the more carbonic acid formed, the more H₂CO₃ dissociates, the more H⁺ ions released, which will combine with the Hb, which will then release its O₂ to go into the respiring cells. This explains the Bohr effect.
The Bohr effect is the release of oxygen from haemoglobin, facilitated by the presence of carbon dioxide. Where CO₂ is high in respiring tissues, oxygen is released more rapidly.
The fate of HCO₃⁻
The HCO₃⁻ diffuses out of the RBC into the plasma where they combine with Na⁺ ions from the dissociation of NaCl to form NaHCO₃.
- It is the inward diffusion of Cl⁻ into the RBC.
- The loss of the negatively charged HCO₃⁻ ion from the RBC is balanced by the inward diffusion of the negative chloride ion (Cl⁻) from the dissociation of NaCl.

- The negativity of HCO₃⁻ ions is compensated by Cl⁻ ion in RBC in equal amount.
- In this way the electrochemical neutrality is restored.

Chloride shift
Mwalimu
Unasoma somo hili? Niulize nikuelezee chochote kilichomo.
Ingia ili kumuuliza Mwalimu wa AI wa Sonza kuhusu mada hii.
Ingia ili kuuliza